Commonly Use DME Modifiers | Durable Medical Equipment Billing Keypoints:
This modifier is used for DME items that are rented, and will be used for equipment in the following categories:
KH — DMEPOS ITEM, INITIAL CLAIM, PURCHASE OR FIRST MONTH RENTAL This modifier is used for a capped rental DME item. When using the KH modifier, you are indicating you are billing for the first month of the capped rental period. KJ — DMEPOS ITEM, PARENTERAL ENTERAL NUTRITION (PEN) PUMP OR CAPPED RENTAL, Month four to fifteen. This modifier is used for capped rental DME items. When using the KJ modifier, you are indicating you are billing for months four through thirteen/fifteen of the capped rental period. KI — DMEPOS ITEM, SECOND OR THIRD MONTH RENTAL This modifier is used for capped rental DME items. When using the KI modifier, you are indicating you are billing for the second and/or third month of the capped rental period A8 — DRESSING FOR EIGHT WOUNDS. (EFFECTIVE DATE 1/1/2003) Surgical dressing codes billed without modifiers A1-A9 (see Coding Guidelines) are noncovered under the Surgical Dressings benefit. Certain dressings may be covered under other benefits. A5 — DRESSING FOR FIVE WOUNDS. (EFFECTIVE DATE 1/1/2003) Surgical dressing codes billed without modifiers A1-A9 (see Coding Guidelines) are noncovered under the Surgical Dressings benefit. Certain dressings may be covered under other benefits. A4 — DRESSING FOR FOUR WOUNDS. (EFFECTIVE DATE 1/1/2003) Surgical dressing codes billed without modifiers A1-A9 (see Coding Guidelines) are noncovered under the Surgical Dressings benefit. Certain dressings may be covered under other benefits. A9 — DRESSING FOR NINE OR MORE WOUNDS. (EFFECTIVE DATE 1/1/2003) Surgical dressing codes billed without modifiers A1-A9 (see Coding Guidelines) are noncovered under the Surgical Dressings benefit. Certain dressings may be covered under other benefits. A1 — DRESSING FOR ONE WOUND. (EFFECTIVE DATE 1/1/2003) Surgical dressing codes billed without modifiers A1-A9 (see Coding Guidelines) are noncovered under the Surgical Dressings benefit. Certain dressings may be covered under other benefits. A7 — DRESSING FOR SEVEN WOUNDS. (EFFECTIVE DATE 1/1/2003) Surgical dressing codes billed without modifiers A1-A9 (see Coding Guidelines) are noncovered under the Surgical Dressings benefit. Certain dressings may be covered under other benefits. A6 — DRESSING FOR SIX WOUNDS. (EFFECTIVE DATE 1/1/2003) Surgical dressing codes billed without modifiers A1-A9 (see Coding Guidelines) are noncovered under the Surgical Dressings benefit. Certain dressings may be covered under other benefits. A3 — DRESSING FOR THREE WOUNDS. (EFFECTIVE DATE 1/1/2003) Surgical dressing codes billed without modifiers A1-A9 (see Coding Guidelines) are noncovered under the Surgical Dressings benefit. Certain dressings may be covered under other benefits. A2 — DRESSING FOR TWO WOUNDS. (EFFECTIVE DATE 1/1/2003) Surgical dressing codes billed without modifiers A1-A9 (see Coding Guidelines) are noncovered under the Surgical Dressings benefit. Certain dressings may be covered under other benefits. KA — ADD ON OPTION/ACCESSORY FOR WHEELCHAIR (EFFECTIVE DATE 01/01/1994) JA — ADMINISTERED INTRAVENOUSLY (EFFECTIVE DATE 01/01/2007) N/A JB — ADMINISTERED SUBCUTANEOUSLY (EFFECTIVE DATE 01/01/2007) For all immune globulin (J1559, J1561, J1562, J1569) and associated infusion pump (E0779) claims where the route of administration is subcutaneous, a JB modifier must be added to each HCPCS code. VP — APHAKIC PATIENT (EFFECTIVE DATE 01/01/1984) N/A TW — BACK-UP EQUIPMENT (EFFECTIVE DATE 01/01/2003) N/A KB — BENEFICIARY REQUESTED UPGRADE FOR ABN, MORE THAN 4 MODIFIERS IDENTIFIED ON CLAIM. (EFFECTIVE DATE 1/1/2003) N/A KT — BENEFICIARY RESIDES IN A COMPETITIVE BIDDING AREA AND TRAVELS OUTSIDE THAT COMPETITIVE BIDDING AREA AND RECEIVES A COMPETITIVE BID ITEM (UPDATED DATE 04/01/2008 N/A KE — BID UNDER ROUND ONE OF THE DMEPOS COMPETITIVE BIDDING PROGRAM FOR USE WITH NON-COMPETITIVE BID BASE EQUIPMENT (EFFECTIVE 01/01/2009) This is a pricing modifier and it used with certain items that may be used with competitive or non-competitive bid items. Use of the KE indicates the 9.5% reduction should not affect your reimbursement. CR — CATASTROPHE/DISASTER RELATED For use by providers that have been granted a formal waiver under §1135 of the Social Security Act and then only for services affected by the emergency and while the waiver remains in effect. QQ — CLAIM SUBMITTED WITH A WRITTEN STATEMENT OF INTENT CT — COMPUTED TOMOGRAPHY SERVICES FURNISHED USING EQUIPMENT THAT DOES NOT MEET EACH OF THE ATTRIBUTES OF THE NATIONAL ELECTRICAL MANUFACTURERS ASSOCIATIONS (NEMA) XR-29-2013 STANDARD N/A PD — DIAGNOSTIC OR RELATED NON DIAGNOSTIC ITEM OR SERVICE PROVIDED IN A WHOLLY OWNED OR OPERATED ENITY TO A PATIENT WHO IS ADMITTED AS AN INPATIENT WITHIN 3 DAYS (EFFECTIVE DATE 01/01/2012) KL — DMEPOS ITEM DELIVERED VIA MAIL (EFFECTIVE DATE 07/01/2007) When using this modifier, you are indicating you have delivered your supplies via mail. This modifier must only be used with diabetic supplies. KG — DMEPOS ITEM SUBJECT TO DMEPOS COMPETITIVE BIDDING PROGRAM NUMBER 1 (EFFECTIVE DATE 07/01/2007) KK — DMEPOS ITEM SUBJECT TO DMEPOS COMPETITIVE BIDDING PROGRAM NUMBER 2 (EFFECTIVE DATE 07/01/2007) KU — DMEPOS ITEM SUBJECT TO DMEPOS COMPETITIVE BIDDING PROGRAM NUMBER 3 (EFFECTIVE DATE 07/01/2007) N/A KW — DMEPOS ITEM SUBJECT TO DMEPOS COMPETITIVE BIDDING PROGRAM NUMBER 4 (EFFECTIVE DATE 1/1/2008) N/A KY — DMEPOS ITEM SUBJECT TO DMEPOS COMPETITIVE BIDDING PROGRAM NUMBER 5 (EFFECTIVE DATE 1/1/2008) N/A KV — DMEPOS ITEM SUBJECT TO DMEPOS COMPETITIVE BIDDING PROGRAM THAT IS FURNISHED AS PART OF A PROFESSIONAL SERVICE (EFFECTIVE DATE 1/1/2008) N/A J4 — DMEPOS ITEM SUBJECT TO DMEPOS COMPETITIVE BIDDING PROGRAM THAT IS FURNISHED BY A HOSPITAL UPON DISCHARGE (EFFECTIVE 01/01/2010) JW — DRUG AMOUNT DISCARDED/NOT ADMINISTERED TO ANY PATIENT (EFFECTIVE 01/01/2003) For CGS DMEMAC claims, the JW modifier is not required for discarded drugs and biologicals. KD — DRUG OR BIOLOGICAL INFUSED THOUGH DME. (EFFECTIVE DATE 01/01/04) RD — DRUG PROVIDED TO BENEFICIARY, BUT NOT ADMINISTERED EM — EMERGENCY RESERVE SUPPLY (FOR ESRD BENEFIT ONLY). ET — EMERGENCY SERVICES EA — ERYTHROPOETIC STIMULATING AGENT (ESA) ADMINISTERED TO TREAT ANEMIA DUE TO ANTI-CANCER CHEMOTHERAPY (EFFECTIVE DATE 1/1/2008) EB — ERYTHROPOETIC STIMULATING AGENT (ESA) ADMINISTERED TO TREAT ANEMIA DUE TO ANTI-CANCER RADIOTHERAPY (EFFECTIVE DATE 1/1/2008) EC — ERYTHROPOETIC STIMULATING AGENT (ESA) ADMINISTERED TO TREAT ANEMIA NOT DUE TO ANTI-CANCER RADIOTHERAPY OR ANTI-CANCER CHEMOTHERAPY (EFFECTIVE DATE 1/1/2008) EX — EXPATRIATE BENEFICIARY Effective July 1, 2016, use this modifier to bill Medicare for purchased only DMEPOS items that are furnished to expatriate beneficiaries. By attaching the EX modifier, the supplier is attesting that the benefidicary is an expatriate beneficiary, and that the item was delivered/furnished while the beneficiary is present in the U.S., and all other billing criteria has been met. QA — FDA INVESTIGATIONAL DEVICE EXEMPTION (ENDS 12/31/2007) KP — FIRST DRUG OF A MULTIPLE DRUG UNIT DOSE FORMULATION When there is a single drug in a unit dose container, the KO modifier is added to the unit dose form code. (Exception: The KO modifier is not used with code J2545 or Q4080.) Except for code J7620, when two or more drugs are combined and dispensed to the patient in the same unit dose container, each of the drugs is billed using its unit dose form code. The KP modifier is added to only one of the unit dose form codes and the KQ modifier is added to the other unit dose code(s). Whenever a unit dose form code is billed, it must have a KO, KP or KQ modifier. (Exception: The KO, KP and KQ modifiers should not be used with code J7620.) If a unit dose code does not have one of these modifiers, it will be denied as an invalid code. The KO, KP, and KQ modifiers are not used with the concentrated form codes. The only FDA-approved unit dose preparation containing more than one drug is J7620, the combination of albuterol and ipratropium. Therefore, if the following FDA-approved unit dose codes are billed with a KP or KQ modifier, they will be rejected as invalid for claim submission: J2545, J7608, J7613, J7614, J7626, J7631, J7639, J7644, J7649, J7659, J7669, J7682, Q4080, and Q4080. RE — FURNISHED IN FULL COMPLIANCE WITH FDA-MANDATED RISK EVALUATION AND MITIGATION STRATEGY (REMS) (EFFECTIVE 01/01/2009) KS — GLUCOSE MONITOR SUPPLY FOR DIABETIC BENEFICIARY NOT TREATED WITH INSULIN If the patient is not being treated with insulin injections, the KS modifier must be added to the code for the monitor and each related supply on every claim submitted. ED — HEMATOCRIT LEVEL HAS EXCEEDED 39% (OR HEMOGLOBIN LEVEL HAS EXCEEDED 13.0 G/DL) FOR 3 OR MORE CONSECUTIVE BILLING CYCLES IMMEDIATELY PRIOR TO AND INCLUDING THE CURRENT CYCLE (EFFECTIVE DATE 1/1/2008) EE — HEMATOCRIT LEVEL HAS NOT EXCEEDED 39% (OR HEMOGLOBIN LEVEL HAS NOT EXCEEDED 13.0 G/DL) FOR 3 OR MORE CONSECUTIVE BILLING CYCLES IMMEDIATELY PRIOR TO AND INCLUDING THE CURRENT CYCLE (EFFECTIVE DATE 1/1/2008) Q0 — INVESTIGATIONAL CLINICAL SERVICE PROVIDED IN A CLINICAL RESEARCH STUDY THAT IS IN AN APPROVED CLINICAL RESEARCH STUDY (EFFECTIVE DATE 1/1/2008) KF — ITEM DESIGNATED BY FDA AS CLASS III DEVICES. (EFFECTIVE DATE 04/01/04) AV — ITEM FURNISHED IN CONJUNCTION WITH A PROSTHETIC DEVICE, PROSTHETIC OR ORTHOTIC. (EFFECTIVE DATE 1/1/2003) AW — ITEM FURNISHED IN CONJUNCTION WITH A SURGICAL DRESSING. (EFFECTIVE DATE 1/1/2003) AU — ITEM FURNISHED IN CONJUNCTION WITH A UROLOGICAL, OSTOMY, OR TRACHEOSTOMY SUPPLY. (EFFECTIVE DATE 1/1/2003) This modifier is used specifically with codes A4450, A4452, and A5120. AX — ITEM FURNISHED IN CONJUNCTION WITH DIALYSIS SERVICES. (EFFECTIVE DATE 1/1/2003) BA — ITEM FURNISHED IN CONJUNCTION WITH PARENTERAL ENTERAL NUTRITION (PEN) SERVICES. (EFFECTIVE DATE 1/1/2003) When an IV pole (E0776) is used in conjunction with parenteral nutrition, the BA modifier should be added to the code. Code E0776 is the only code with which the BA modifier may be used. GZ — ITEM OR SERVICE EXPECTED TO BE DENIED AS NOT REASONABLE OR NECESSARY. (EFFECTIVE 1/1/2002) AY — ITEM OR SERVICE FURNISHED TO AN ESRD PATIENT THAT IS NOT FOR THE TREATMENT OF ESRD (EFFECTIVE 01/01/2011) QV — ITEM OR SERVICE PROVIDED AS ROUTINE CARE IN A MEDICARE QUALIFYING CLINICAL TRAIL (ENDS 12/31/2007) GY — ITEM OR SERVICE STATUTORILY EXCLUDED, DOES NOT MEET THE DEFINITION OF ANY MEDICARE BENEFIT OR, FOR NON-MEDICARE INSURERS, IS NOT A CONTRACT BENEFIT (UPDATED 1/1/2008) FB — ITEM PROVIDED W/O COST TO PROVIDER, SUPPLIER OR PRACTITIONER, OR FULL CREDIT RECEIVED FOR REPLACED DEVICE (UPDATED 1/1/2008) QR — ITEM/SERVICE IN MEDICARE STUDY - OXYGEN (ENDS 12/31/2007) T4 — LEFT FOOT, FIFTH DIGIT (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1830 or E1831. Failure to append the modifier will result in a rejection for incorrect coding. T3 — LEFT FOOT, FOURTH DIGIT (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1830 or E1831. Failure to append the modifier will result in a rejection for incorrect coding. TA — LEFT FOOT, GREAT TOE (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1830 or E1831. Failure to append the modifier will result in a rejection for incorrect coding. T1 — LEFT FOOT, SECOND DIGIT (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1830 or E1831. Failure to append the modifier will result in a rejection for incorrect coding. T2 — LEFT FOOT, THIRD DIGIT (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1830 or E1831. Failure to append the modifier will result in a rejection for incorrect coding. F3 — LEFT HAND, FOURTH DIGIT (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1825. Failure to append the modifier will result in a rejection for incorrect coding. F1 — LEFT HAND, SECOND DIGIT (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1825. Failure to append the modifier will result in a rejection for incorrect coding. F2 — LEFT HAND, THIRD DIGIT (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1825. Failure to append the modifier will result in a rejection for incorrect coding. FA — LEFT HAND, THUMB (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1825. Failure to append the modifier will result in a rejection for incorrect coding. LT — LEFT SIDE. (USED TO IDENTIFY ITEM PROVIDED FOR THE LEFT SIDE OF THE BODY.) N/A K0 — LOWER EXTREMITY PROSTHESIS FUNCTIONAL LEVEL 0 DOES NOT HAVE THE ABILITY OR POTENTIAL TO AMBULATE OR TRANSFER SAFELY WITH OR WITHOUT ASSISTANCE AND A PROSTHESIS DOES NOT ENHANCE THEIR QUALITY OF LIFE OR MOBILITY. K1 — LOWER EXTREMITY PROSTHESIS FUNCTIONAL LEVEL 1 HAS THE ABILITY OR POTENTIAL TO USE A PROSTHESIS FOR TRANSFERS OR AMBULATION ON LEVEL SURFACES AT FIXED CADENCE. TYPICAL OF THE LIMITED AND UNLIMITED HOUSEHOLD AMBULATOR. K2 — LOWER EXTREMITY PROSTHESIS FUNCTIONAL LEVEL 2 HAS THE ABILITY OR POTENTIAL FOR AMBULATION WITH THE ABILITY TO TRAVERSE LOW LEVEL ENVIRONMENTAL BARRIERS SUCH AS CURBS, STAIRS OR UNEVEN SURFACES. TYPICAL OF THE LIMITED COMMUNITY AMBULATOR. K3 — LOWER EXTREMITY PROSTHESIS FUNCTIONAL LEVEL 3 HAS THE ABILITY OR POTENTIAL FOR AMBULATION WITH VARIABLE CADENCE. TYPICAL OF THE COMMUNITY AMBULATOR WHO HAS THE ABILITY TO TRANSVERSE MOST ENVIRONMENTAL BARRIERS AND MAY HAVE VOCATIONAL, THERAPEUTIC OR EXERCISE ACTIVITY THAT DEMANDS PROSTHETIC UTILIZATION BEYOND SIMPLE LOCOMOTION. K4 — LOWER PROSTHESIS FUNCTIONAL LEVEL 4 HAS THE ABILITY OR POTENTIAL FOR PROSTHETIC AMBULATION THAT EXCEEDS THE BASIC AMBULATION SKILLS, EXHIBITING HIGH IMPACT, STRESS, OR ENERGY LEVELS, TYPICAL OF THE PROSTHETIC DEMANDS OF THE CHILD, ACTIVE ADULT, OR ATHLETE. SC — MEDICALLY NECESSARY SERVICE OR SUPPLY (EFFECTIVE DATE 01/01/2001) GL — MEDICALLY UNNECESSARY UPGRADE PROVIDED INSTEAD OF NON-UPGRADED ITEM, NO CHARGE, NO ADVANCE BENEFICIARY NOTICE (ABN) (UPDATED 1/1/2008) M2 — MEDICARE SECONDARY PAYER (MSP) (EFFECTIVE DATE 01/01/2007) 99 — MODIFIER OVERFLOW. (EFFECTIVE DATE 7/1/2003) This modifier is used when you have exhausted the modifier field on the claim form. If you need additional room to add modifiers, append the 99 modifier to the last available field and include a narrative of other modifiers needed on the claim. NB — NEBULIZER SYSTEM, ANY TYPE, FDA-CLEARED FOR USE WITH SPECIFIC DRUG (EFFECTIVE 01/01/2011) NU — NEW DURABLE MEDICAL EQUIPMENT PURCHASE. This modifier is used for new DME items that are purchased. When using the NU modifier, you are indicating you have furnished the beneficiary with a new (never used) piece of equipment. NR — NEW WHEN RENTED EY — NO PHYSICIAN OR OTHER LICENSED HEALTH CARE PROVIDER ORDER FOR THIS ITEM OR SERVICE. (EFFECTIVE DATE 1/1/2003) If you do not have a prescription from the physician prior to billing Medicare, you must append the EY modifier to your claim GX — NOTICE OF LIABILITY ISSUED, VOLUNTARY UNDER PAYER POLICY (EFFECTIVE 04/01/2010) ZA — NOVARTIS/SANDOZ BO — ORALLY ADMINISTERED NUTRITION, NOT BY FEEDING TUBE. (EFFECTIVE DATE 1/1/2003) When enteral nutrients (B4149-B4162) are administered by mouth, the BO modifier must be added to the code. QH — OXYGEN CONSERVING DEVICE IS BEING USED WITH AN OXYGEN DELIVERY SYSTEM. FC — PARTIAL CREDIT RECEIVED FOR REPLACED DEVICE (EFFECTIVE DATE 1/1/2008) CG — POLICY CRITERIA APPLIED (EFFECTIVE DATE 07/01/2008) Effective for claims with dates of service on or after July 1, 2010, if an L3923 orthosis has a rigid plastic or metal component, the supplier must add the CG modifier (policy criteria applied) to the code. Claims for L3923 billed without a CG modifier will be rejected as incorrect coding. The CG modifier must be added to code L0450, L0454, L0455, L0621, L0625, or L0628 only if it is one made primarily of nonelastic material (e.g., canvas, cotton or nylon) or having a rigid posterior panel. QF — PRESCRIBED AMOUNT OF OXYGEN EXCEEDS 4 LPM AND PORTABLE OXYGEN IS PRESCRIBED. These modifiers may only be used with stationary gaseous (E0424) or liquid (E0439) systems or with an oxygen concentrator (E1390, E1391). They must not be used with codes for portable systems or oxygen contents. QG — PRESCRIBED AMOUNT OF OXYGEN IS GREATER THAN 4 LITERS PER MINUTE (LPM). These modifiers may only be used with stationary gaseous (E0424) or liquid (E0439) systems or with an oxygen concentrator (E1390, E1391). They must not be used with codes for portable systems or oxygen contents. QE — PRESCRIBED AMOUNT OF OXYGEN IS LESS THAN 1 LITER PER MINUTE (LPM). This modifier may only be used with stationary gaseous (E0424) or liquid (E0439) systems or with an oxygen concentrator (E1390, E1391). They must not be used with codes for portable systems or oxygen contents CC — PROCEDURE CODE CHANGE (USE 'CC' WHEN THE PROCEDURE CODE SUBMITTED WAS CHANGED EITHER FOR ADMINISTRATIVE REASONS OR BECAUSE AN INCORRECT CODE WAS FILED). (SUPPLIERS SHOULD NOT SUBMIT MODIFIER CC.) PL — PROGRESSIVE ADDITION LENSES (EFFECTIVE DATE 01/01/89) GK — REASONABLE AND NECESSARY ITEM/SERVICE ASSOCIATED WITH A GA OR GZ MODIFIER (UPDATED 1/1/2008) KR — RENTAL ITEM, BILLING FOR PARTIAL MONTH. RP — REPLACEMENT AND REPAIR. (DELETED EFFECTIVE 12/31/2008) RP MAY BE USED TO INDICATE REPLACEMENT OF DME, ORTHOTIC AND PROSTHETIC DEVICES, WHICH HAVE BEEN IN USE FOR SOMETIME. RA — REPLACEMENT OF A DME ITEM (EFFECTIVE 01/01/2009) Claims for replacement of DME items should include the RA modifer for dates of service on or after January 1, 2009. RB — REPLACEMENT OF A PART OF DME FURNISHED AS PART OF A REPAIR (EFFECTIVE 01/01/2009) KM — REPLACEMENT OF FACIAL PROSTHESIS INCLUDING NEW IMPRESSION/MOULAGE KN — REPLACEMENT OF FACIAL PROSTHESIS USING PREVIOUS MASTER MODEL KC — REPLACEMENT OF SPECIAL POWER WHEELCHAIR INTERFACE. (EFFECTIVE DATE 01/01/05) T9 — RIGHT FOOT, FIFTH DIGIT (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1830 or E1831. Failure to append the modifier will result in a rejection for incorrect coding. T8 — RIGHT FOOT, FOURTH DIGIT (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1830 or E1831. Failure to append the modifier will result in a rejection for incorrect coding. T5 — RIGHT FOOT, GREAT TOE (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1830 or E1831. Failure to append the modifier will result in a rejection for incorrect coding. T6 — RIGHT FOOT, SECOND DIGIT (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1830 or E1831. Failure to append the modifier will result in a rejection for incorrect coding. T7 — RIGHT FOOT, THIRD DIGIT (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1830 or E1831. Failure to append the modifier will result in a rejection for incorrect coding. F9 — RIGHT HAND, FIFTH DIGIT (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1825. Failure to append the modifier will result in a rejection for incorrect coding. F8 — RIGHT HAND, FOURTH DIGIT (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1825. Failure to append the modifier will result in a rejection for incorrect coding. F6 — RIGHT HAND, SECOND DIGIT (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1825. Failure to append the modifier will result in a rejection for incorrect coding. F7 — RIGHT HAND, THIRD DIGIT (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1825. Failure to append the modifier will result in a rejection for incorrect coding. F5 — RIGHT HAND, THUMB (EFFECTIVE DATE 01/01/1995) Effective for dates of service on or after January 1, 2015, use with devices coded with HCPCS code E1825. Failure to append the modifier will result in a rejection for incorrect coding. RT — RIGHT SIDE (USED TO IDENTIFY PROCEDURES PERFORMED ON THE RIGHT SIDE OF THE BODY). Q1 — ROUTINE CLINICAL SERVICE PROVIDED IN A CLINICAL RESEARCH STUDY THAT IS IN AN APPROVED CLINICAL RESEARCH STUDY (EFFECTIVE DATE 1/1/2008) KQ — SECOND OR SUBSEQUENT DRUG OF A MULTIPLE DRUG UNIT DOSE FORMULATION When there is a single drug in a unit dose container, the KO modifier is added to the unit dose form code. (Exception: The KO modifier is not used with code J2545 or Q4080.) Except for code J7620, when two or more drugs are combined and dispensed to the patient in the same unit dose container, each of the drugs is billed using its unit dose form code. The KP modifier is added to only one of the unit dose form codes and the KQ modifier is added to the other unit dose code(s). Whenever a unit dose form code is billed, it must have a KO, KP or KQ modifier. (Exception: The KO, KP and KQ modifiers should not be used with code J7620.) If a unit dose code does not have one of these modifiers, it will be denied as an invalid code. The KO, KP, and KQ modifiers are not used with the concentrated form codes. The only FDA-approved unit dose preparation containing more than one drug is J7620, the combination of albuterol and ipratropium. Therefore, if the following FDA-approved unit dose codes are billed with a KP or KQ modifier, they will be rejected as invalid for claim submission: J2545, J7608, J7613, J7614, J7626, J7631, J7639, J7644, J7649, J7659, J7669, J7682, Q4080, and Q4080. GW — SERVICE NOT RELATED TO THE HOSPICE PATIENT'S TERMINAL CONDITION. (USED FOR MEDICARE ADVANTAGE PLANS CLAIMS) QJ — SERVICE/ITEMS PROVIDED TO A PRISONER OR PATIENT IN STATE OR LOCAL CUSTODY, HOWEVER THE STATE OR LOCAL GOVERNMENT, AS APPLICABLE, MEETS THE REQUIREMENT IN 42 CFR 411.1(B). (EFFECTIVE DATE 1/1/2003) KO — SINGLE DRUG UNIT DOSE FORMULATION When there is a single drug in a unit dose container, the KO modifier is added to the unit dose form code. (Exception: The KO modifier is not used with code J2545 or Q4080.) Except for code J7620, when two or more drugs are combined and dispensed to the patient in the same unit dose container, each of the drugs is billed using its unit dose form code. The KP modifier is added to only one of the unit dose form codes and the KQ modifier is added to the other unit dose code(s). Whenever a unit dose form code is billed, it must have a KO, KP or KQ modifier. (Exception: The KO, KP and KQ modifiers should not be used with code J7620.) If a unit dose code does not have one of these modifiers, it will be denied as an invalid code. The KO, KP, and KQ modifiers are not used with the concentrated form codes. The only FDA-approved unit dose preparation containing more than one drug is J7620, the combination of albuterol and ipratropium. Therefore, if the following FDA-approved unit dose codes are billed with a KP or KQ modifier, they will be rejected as invalid for claim submission: J2545, J7608, J7613, J7614, J7626, J7631, J7639, J7644, J7649, J7659, J7669, J7682, Q4080, and Q4080. MS — SIX MONTH MAINTENANCE AND SERVICING FEE FOR REASONABLE AND NECESSARY PARTS AND LABOR WHICH ARE NOT COVERED UNDER ANY MANUFACTURER OR SUPPLIER WARRANTY For capped rental periods beginning prior to January 1, 2006 which have reached the 15 month rental cap, DME MACs pay claims for maintenance and servicing fees after six months have passed from the end of the final paid rental month or from the end of the period the item is no longer covered under the supplier's or manufacturer's warranty, whichever is later. A new CMN and/or physician's order is not needed for covered maintenance. KX — SPECIFIC REQUIRED DOCUMENTATION ON FILE. (EFFECTIVE DATE 7/1/2002) This modifier may be used to indicate that specific required documentation is on file in the patient's medical record. Documentation must be submitted upon request. Applicable policies include: Manual and power mobility bases and accessories, Glucose monitors & supplies, PAP devices and accessories, Respiratory Assist Devices (RAD), Commodes, Hospital beds and accessories, Therapeutic Shoes for Diabetics, Heavy duty walkers, Urological Supplies, Epoetin, Support surfaces - Groups 1, 2, and 3, Refractive Lenses - Anti reflective coating, tint, and oversize lenses, polycarbonate lenses, Cervical Traction devices - Codes E0849 and E0855, External infusion (insulin) pumps, High Frequency chest wall oscillation devices, Nebulizers (Brovana or Perforomist) - J7605 and J7606, Negative Pressure Wound Therapy, Patient lifts - E0636 and E1035, Speech generating devices, Wheelchair seating, Orthopedic Footwear, Home Dialysis supplies, Oral Antiemetic - J8502 and J8540. EJ — SUBSEQUENT CLAIMS FOR A DEFINED COURSE OF THERAPY, E.G., EPO, SODIUM HYALURONATE, INFLAXIMAB. BU — THE BENEFICIARY HAS BEEN INFORMED OF THE PURCHASE AND RENTAL OPTIONS AND AFTER 30 DAYS HAS NOT INFORMED THE SUPPLIER OF HIS/HER DECISION. This modifier is used when you have discussed the purchase/rent option with the beneficiary, and the beneficiary has not responded within 30 days of the discussion. BP — THE BENEFICIARY HAS BEEN INFORMED OF THE PURCHASE AND RENTAL OPTIONS AND HAS ELECTED TO PURCHASE THE ITEM. This modifier is used when you have discussed the purchase/rent option with the beneficiary, and the beneficiary has chosen to purchase the DME item. BR — THE BENEFICIARY HAS BEEN INFORMED OF THE PURCHASE AND RENTAL OPTIONS AND HAS ELECTED TO RENT THE ITEM. This modifier is used when you have discussed the purchase/rent option with the beneficiary, and the beneficiary has chosen to rent the DME item. GD — UNITS OF SERVICE EXCEEDS MEDICALLY UNLIKELY EDIT VALUE AND REPRESENTS REASONABLE AND NECESSARY SERVICES (EFFECTIVE DATE 1/1/2008) UE — USED DURABLE MEDICAL EQUIPMENT PURCHASE. This modifier is used for used DME items that are purchased. When using the UE modifier, you are indicating you have furnished the beneficiary with a used piece of equipment. GU — WAIVER OF LIABILITY STATEMENT ISSUED AS REQUIRED BY PAYER POLICY, ROUTINE NOTICE (EFFECTIVE 01/01/2011) GA — WAIVER OF LIABILITY STATEMENT ON FILE. You must fully execute the Advanced Beneficiary Notice before appending the GA modifier to your claim. In order to have the GA modifier added to your claim after the initial determination, you must submit the ABN in paper to Written Reopenings. Sample of HCFA 1500 Claim Form when billing for DME Billing 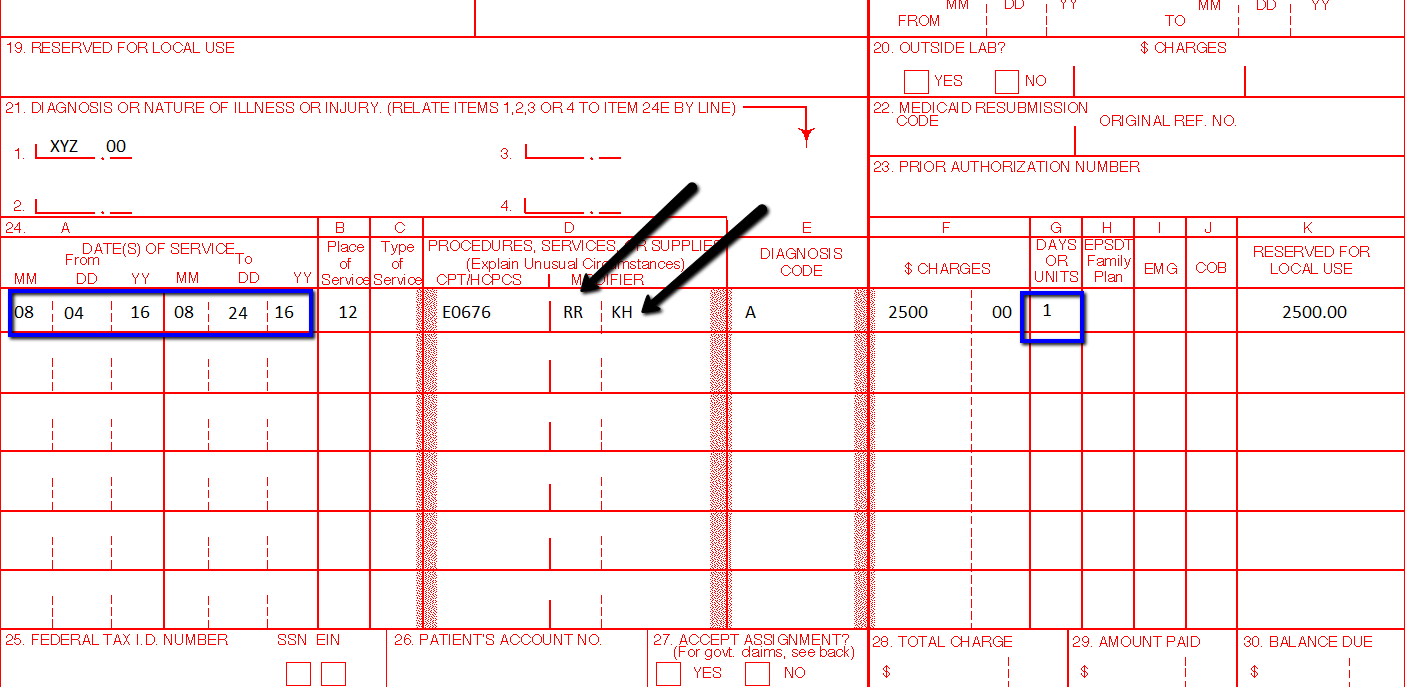 Searched Keywords:
dme modifier list 2016 dme procedure code list medicare dme modifiers list purchase modifier for dme dme modifiers medicare dme cpt codes dme modifiers hcpcs list of D Durable Medical what is durable medical equipment durable equipment definition durable equipment providers durable medical equipment near me dme medicare modifiers dme modifier kx dme modifiers 2017 dme modifiers 2016 dme purchase modifier medicare dme modifiers 2016 medicare modifiers list what is the kx modifier used for? dme rental modifiers modifier kh dme modifiers list dme modifier kx dme modifiers 2016 medicare dme modifiers 2016 dme modifiers 2017 modifier bp
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |

ABOUT THE AUTHOR:
Ms. Pinky Maniri-Pescasio is the Founder of GoHealthcare Consulting. She is a National Speaker on Practice Reimbursement and a Physician Advocate. She has served the Medical Practice Industry for more than 25 years as a Professional Medical Practice Consultant. 
search hereArchives
July 2024
Categories
All
BROWSE HERE
All
|
- About
- Leadership
- Contact Us
- Testimonials
- READ OUR BLOG
-
Let's Meet in Person
- 2023 ORTHOPEDIC VALUE BASED CARE CONFERENCE
- 2023 AAOS Annual Meeting of the American Academy of Orthopaedic Surgeons
- 2023 ASIPP 25th Annual Meeting of the American Society of Interventional Pain Management
- 2023 Becker's 20th Annual Spine, Orthopedic & Pain Management-Driven ASC Conference
- 2023 FSIPP Annual Conference by FSIPP FSPMR Florida Society Of Interventional Pain Physicians
- 2023 New York and New Jersey Pain Medicine Symposium
- Frequently Asked Questions and Answers - GoHealthcare Practice Solutions
- Readers Questions
 RSS Feed
RSS Feed
Photos from shixart1985 (CC BY 2.0), www.ilmicrofono.it, shixart1985